👉👉 🇺🇸 All Posts 🇬🇧 / 🇯🇵 記事一覧 🇯🇵 👈👈
♦️ Disclaimer
I must admit, physics is not my strong point 😅.
I am aware that the underlying physical phenomena are complex and cannot always be explained in a simple way.
This article focuses on easy-to-grasp concepts rather than strict physical accuracy. Please forgive any oversimplifications or parts that are not 100% precise.
♦️ Timing of Wheeze / Stridor
In patients with upper airway obstruction (e.g., tongue falling back under sedation, obstructive sleep apnea), wheezing sounds are typically heard during inspiration. The typical sound of upper airway obstruction is called stridor.
In contrast, in lower airway obstruction (e.g., asthma, bronchospasm, severe emphysema), wheezing is heard during expiration. The typical sound here is called a wheeze.
So why does this difference occur?
(And by the way, in severe cases of either disease, both inspiratory and expiratory wheeze can be heard.)
♦️ Wheeze occurs when airflow passes through a narrowed segment, creating turbulance.
Imagine water running through a garden hose. If you pinch the hose, the velocity of water increases, right? Did you ever play with this as a kid—or during cleaning? No? Just me? 😅
Air behaves the same way. When airflow encounters a narrowed passage, its velocity increases, creating turbulence. This turbulence causes the airway wall to vibrate, which then produces vibration in the surrounding air, and this is what we perceive as wheezing sounds.
👉 Note: Wheeze is not just turbulence. It is turbulence plus airway wall vibration, and that vibration is the true source of the sound.
🔷 Normal inspiration and expiration schema
In healthy subjects, airflow during inspiration and expiration remains smooth, without turbulence.
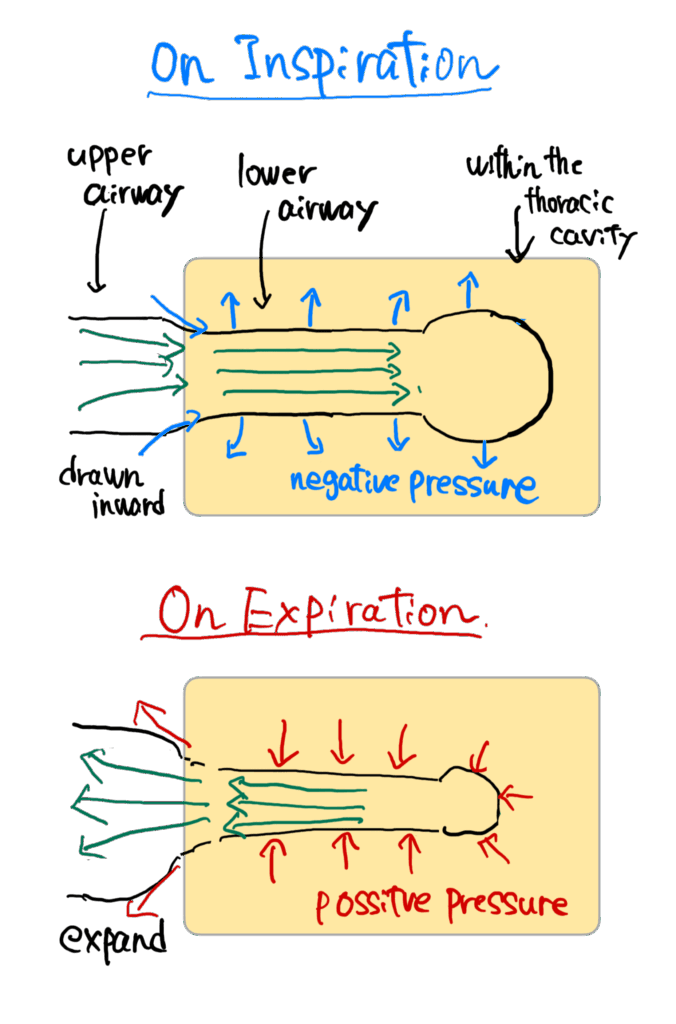
Green arrows = airflow.
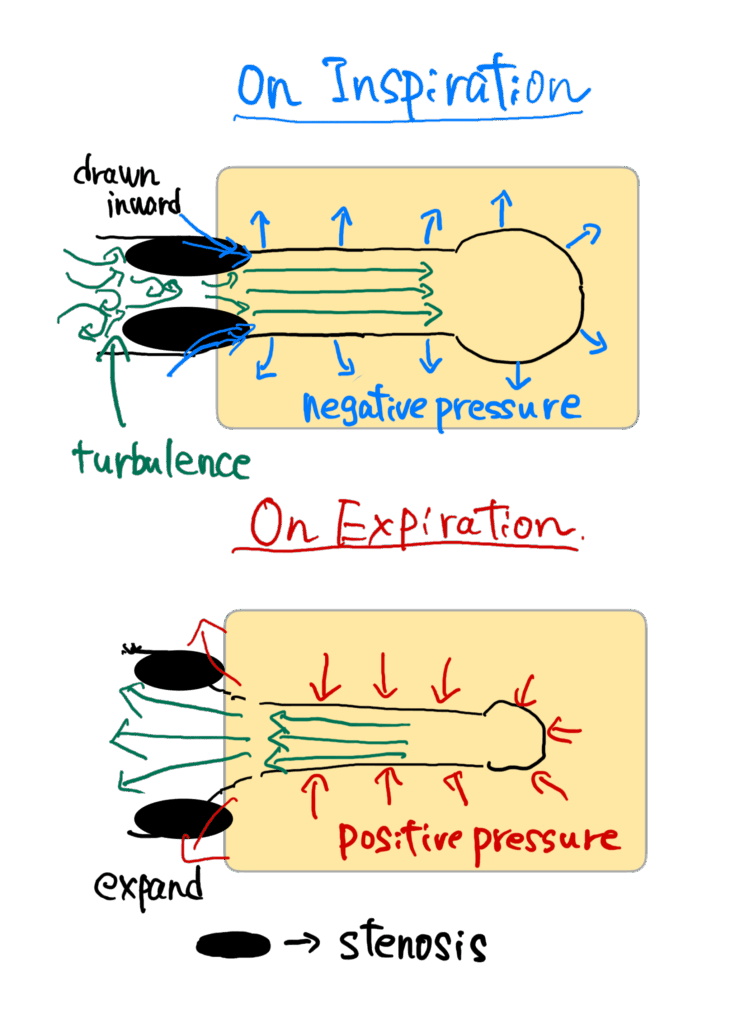
🔷 Upper airway obstruction: Why inspiratory stridor occurs
The upper airway (pharynx, larynx, vocal cords) is mainly composed of soft tissue.
During inspiration, diaphragmatic contraction creates a negative intrathoracic (airway) pressure, drawing air inward. Because these tissues are soft, they are pulled inward, narrowing the airway even further. As a result, airflow accelerates through the narrowed lumen, generating turbulence and stridor.
Normally, slight narrowing doesn’t cause audible stridor, but in conditions like OSA or sedation-induced tongue base collapse, strong turbulence occurs.
During expiration, however, intrathoracic pressure becomes positive, pushing outward and helping the upper airway open. Air moves from a narrower space (bronchi) into the wider upper airway, so turbulence is less likely, and expiratory stridor is uncommon.
But if obstruction is severe, airflow generates strong turbulence in both phases, and biphasic stridor can be heard.
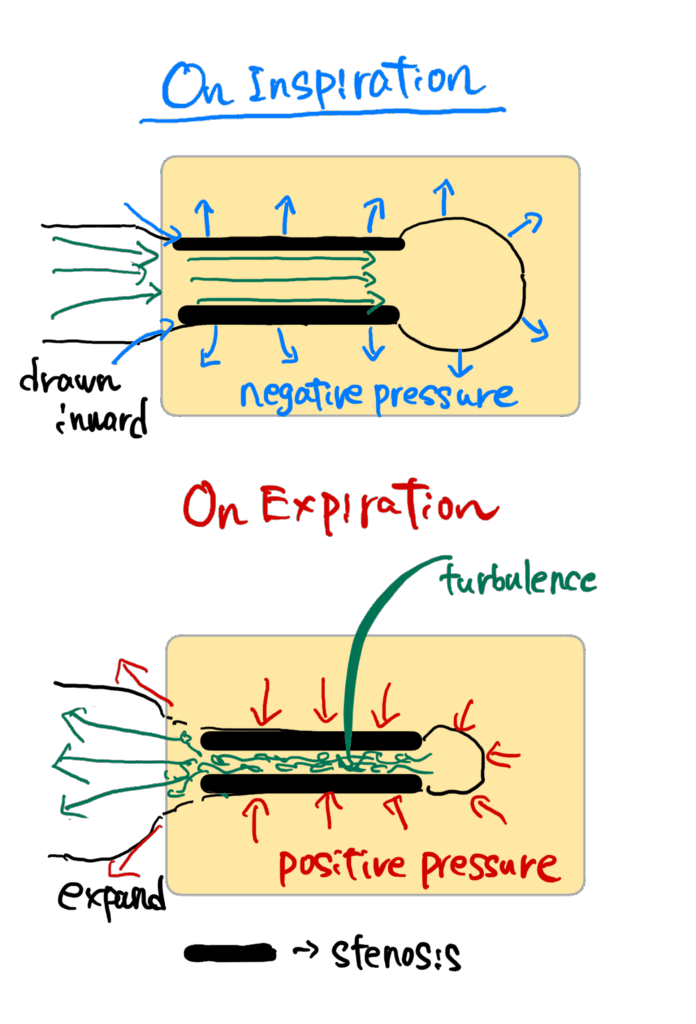
🔷 Lower airway obstruction: Why expiratory wheeze occurs
In asthma attacks or emphysema, lower airway narrowing is present. During expiration, intrathoracic pressure rises, compressing alveoli and small airways. Air must pass through these narrowed bronchioles, producing turbulence and wheeze.
One might expect turbulence during inspiration as well, since airways are already narrowed by chronic inflammation. However, the negative intrathoracic pressure of inspiration pulls the bronchi outward, expanding them slightly. This makes turbulence less pronounced during inspiration—unless the obstruction is severe.
👉 Note: Expiratory wheeze is accentuated not only by positive pressure compressing the bronchioles, but also by inflammation, edema, and mucus narrowing the airway lumen.
📝 Summary ( Take home points )
- Wheeze/stridor occurs when airflow passes through a narrowed airway segment, causing turbulence and airway wall vibration.
- Upper airway obstruction:
- Inspiratory negative pressure narrows the soft tissue airway → turbulence → inspiratory stridor.
- Expiration widens the upper airway → expiratory stridor is less common.
- Severe cases → biphasic stridor.
- Lower airway obstruction:
- Inspiration expands bronchioles → less turbulence.
- Expiration compresses bronchioles + inflammation/secretions → turbulence → expiratory wheeze.
- Severe cases → inspiratory wheeze as well.
- Stridor: high-pitched, upper airway.
- Wheeze: may be high-pitched or low-pitched, typically expiratory, from lower airways.
🔗 Related articles
- Coming soon
📚 References & Further reading
- Global Initiative for Asthma (GINA) 2024 — Summary Guide 🔗 GINA 2024 PDF → Describes wheeze as a typical feature of asthma, often heard during forced expiration due to expiratory airflow limitation. Supports the explanation of lower airway obstruction and expiratory wheeze.
- Merck Manuals — “Stridor — Pulmonary Disorders” 🔗 Merck Manual Professional Edition → Defines stridor as a sound generated by “rapid, turbulent flow of air through a narrowed or partially obstructed segment of the extrathoracic upper airway.” Supports the section on upper airway obstruction and inspiratory stridor.
- StatPearls — “Stridor in Children” (2023, NCBI Bookshelf) 🔗 NCBI Bookshelf → Explains that stridor is a high-pitched sound produced by irregular airflow through a narrowed upper airway, most commonly during inspiration. Provides additional context for understanding the mechanics of upper airway obstruction.
コメントを投稿するにはログインしてください。