🔷 Introduction
Functional Residual Capacity (FRC) is one of those terms that anyone who has studied anesthesia, pulmonary physiology, or even basic respiratory function testing has come across.
We know from textbooks and daily practice:
- General anesthesia decreases FRC.
- Obesity and pregnancy decrease FRC.
- Supine position decreases FRC.
These reductions predispose patients to atelectasis and hypoxemia. Let’s break it down.
🔷 What is Residual Volume (RV)?
Residual volume (RV) is the amount of air that remains in the lungs after a maximal exhalation. Even if you blow out as hard as you can, the lungs never collapse into a vacuum. RV prevents alveolar collapse and keeps the lungs “propped open.”
🔷 What is FRC and how does it differ?
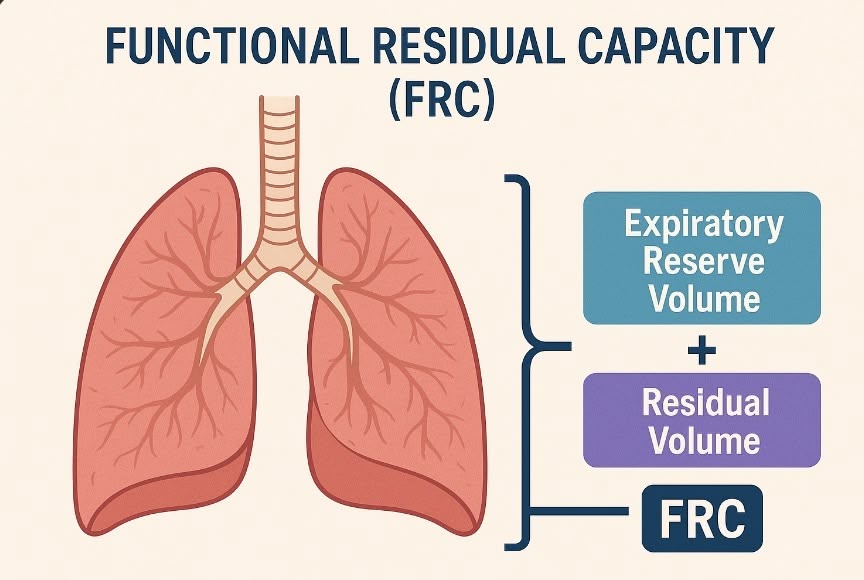
FRC is the volume of air left in the lungs at the end of a normal tidal expiration.
- Formula: FRC = RV + Expiratory Reserve Volume (ERV)
- It represents the equilibrium point where the inward elastic recoil of the lungs balances the outward recoil of the chest wall.
Unlike vital capacity or tidal volume, FRC cannot be measured directly by spirometry. It requires specialized methods such as:
- Helium dilution
- Nitrogen washout
- Body plethysmography
🔷 How much is it?
In healthy adults, FRC is usually around 2.5–3.0 liters in the upright position, or approximately 30 mL/kg of ideal body weight.
Note: In obesity, FRC does not increase with body weight; in fact, it decreases.
🔷 Why is it called “Functional”?
Think of FRC as your intrathoracic oxygen reserve—a built-in oxygen tank.👍
When you stop breathing, you don’t immediately desaturate because oxygen is still available from:
- Oxygen bound to hemoglobin
- Oxygen stored in the FRC
This is why preoxygenation (replacing nitrogen in the FRC with oxygen) is so critical—it increases the “safe apnea time.” Strategies like PEEP, CPAP, or head-up positioning can increase FRC and further extend this window.
🔷 Factors that Reduce FRC
As stated abobe..
- General anesthesia: ↓ by ~20% shortly after induction.
- Supine position: ↓ by ~20–25% compared with upright sitting. Trendelenburg worsens the effect.
- Pregnancy: ↓ by ~10–25% due to reduced ERV and RV.
- Obesity: FRC decreases exponentially with rising BMI. In severe obesity, FRC may approach or fall below the closing capacity (CC), leading to airway closure and atelectasis.
🔷 Clinical Implications
When FRC < closing capacity, small airway closure occurs in dependent lung regions, causing:
- Ventilation–perfusion mismatch
- Absorptive atelectasis
- Hypoxemia
This is why atelectasis is common after induction of anesthesia, especially in obese, pregnant, elderly, or supine patients.
Optimizing FRC through preoxygenation, PEEP, recruitment maneuvers, and positioning is essential in perioperative management.
📝 Summary
📝 Summary
- Definition: FRC = RV + ERV, the lung volume at end-tidal expiration, where lung and chest wall elastic forces balance.
- Normal value: ~2.5–3.0 L (≈30 mL/kg IBW) in upright healthy adults.
- Measurement: Not measurable by spirometry; requires helium dilution, nitrogen washout, or body plethysmography.
- Clinical relevance: General anesthesia, supine position, obesity, and pregnancy all reduce FRC, increasing the risk of atelectasis and hypoxemia.
- Key intervention: Preoxygenation maximizes the FRC’s oxygen reservoir, extending safe apnea time.
🔗 Related articles
📚 References & Links
- StatPearls: Functional Residual Capacity
- StatPearls: Atelectasis
- Wahba RW. Perioperative functional residual capacity.
- Hedenstierna G. Effects of anesthesia on the respiratory system.
- LoMauro A, Aliverti A. Respiratory physiology of pregnancy.
- Peters U et al. Effect of obesity on lung function.
- Smith LJ et al. Supine posture changes lung volumes…
コメントを投稿するにはログインしてください。